Cardiovascular health in patients with MPNs
- Introduction
- What is cardiovascular disease (CVD)?
- Most common types of cardiovascular disease
- Main CVD risk factors for MPN patients
- Thrombosis
- Heart attack and stroke risk
- Heart failure
- Pulmonary hypertension
- Electrical problems Whilst not as well studied, there is some evidence that atrial fibrillation (AF), a common electrical problem, may be more prevalent in MPN patients. But further research is needed.
- Managing cardiovascular risk factors in MPN patients
NOTE: The work of two US cardiologists (Dr Stephanie Feldman and Dr Orly Leiva) has informed this webpage. Both have researched the emerging field of the relationship between cardiovascular health and MPNs.
This page also features information from Australian haematologist, Dr Cecily Forsyth who has a special interest in MPNs and whose ongoing support to MPN patients and the MPN AA is immeasurable.
Introduction
It is very important for MPN patients to maintain good cardiovascular health. Cardiovascular disease is a leading cause of morbidity (illness) and mortality in patients with MPNs.
US cardiologist Dr Stephanie Feldman explains:
‘Like other patients with cancer, patients with MPN are at increased risk for cardiovascular disease…..‘As a patient living with MPN, this information is not meant to scare you, but instead to empower you to work with your care team to get the best possible treatment for your MPN while minimizing the short and long term risks to your heart.’
Dr Feldman recommends ‘ In order to protect your heart and prevent cardiovascular disease, just follow the ABCDEs of cardiovascular health.’
Her full video presentation is HERE (courtesy of CR&T 2024)
US cardiologist Dr Orly Leiva
Dr Leiva has researched MPNs and cardiovascular disease for several years. His research highlights that although thrombosis is a well-established risk factor in MPNs, non-thrombotic conditions, including heart failure and pulmonary hypertension, are also prevalent, especially in myelofibrosis patients.
His 2025 video presentation HERE is especially relevant for patients with myelofibrosis. He explains that an MPN is not only a chronic haematological disease mainly managed by haematologists, but rather, an MPN is ‘a systemic disorder that affects the whole body. And cardiovascular diseases, in particular, are very important when it comes to prognosis and morbidity in patients with MPNs.’
Dr Leiva recommends that all MPN patients aged 50 and over seek to have an appointment with a cardiologist.
What is cardiovascular disease (CVD)?
Cardiovascular disease is a term for conditions that affect:
– the heart,
– the blood vessels (arteries and veins), and
– the electrical system (tells heart when and how to beat).
Cardiovascular disease can be considered as:
– pump problems (stiff, weak heart, congestive heart failure, valve problems, high blood pressure going to the lungs -known as pulmonary hypertension),
– plumbing problems (coronary artery disease, heart attack, peripheral arterial disease, cerebrovascular disease), and
– electricity problems (arrhythmias, atrial fibrillation, heart block).
Most common types of cardiovascular disease
- Coronary artery disease – the most common form – where arteries supplying the heart become narrowed by cholesterol plaques which can cause chest pain (angina) or heart attacks.
- Heart attack (myocardial infarction) – a sudden, complete or partial blockage of a heart artery (usually a clot on a plaque) and so part of the heart muscle is damaged or dies.
- Stroke – blood flow to the brain is interrupted causing a clot (ischemic stroke) or bleeding (haemorrhagic stroke).
- Heart failure –Heart failure occurs when the heart is unable to pump blood efficiently throughout the body. This can be due to a weak heart that is unable to pump sufficient blood forward or a stiff heart that pumps well but is unable to fill adequately. This can lead to inadequate blood flow to organs and backing up of blood into the venous system causing congesting of veins and accumulation of fluid in the lungs (pulmonary oedema), legs (peripheral oedema), and abdomen (ascites). Risk factors in the general population include prior heart attacks, diabetes, high blood pressure, family history/genetics, obesity, or heart valve disease.
- Arrhythmias (an electrical problem) – abnormal heart rhythms (too fast, too slow, or irregular). Some can be harmless, but some increase stroke risk.
Main CVD risk factors for MPN patients
Most CVD develops from atherosclerosis which is a slow, decades long process:
– cholesterol plus inflammation builds up in artery walls;
– this causes arteries to become stiff and narrow; and
– plaques can rupture which leads to clots forming.
Some risk factors can’t be altered, such as: age; sex; genetics.
But most can be managed, such as smoking, being overweight, having an unhealthy diet, lack of physical activity, high blood pressure, high cholesterol, uncontrolled diabetes. Electrical problems of the heart should also be managed – eg atrial fibrillation, arrythmias.
Below are the main cardiovascular risk factors that haematologists look out for and to manage in their MPN patients
Australian haematologist Dr Cecily Forsyth presented on thrombosis (blood clots) at the MPN symposium in October 2025.
Her presentation slides and video describe specific concerns for MPN patients and how to manage them.
Myelofibrosis patients and thrombosis – MF patients need nuanced treatment in managing thrombosis and cardiovascular disease. For more information about this topic and thrombosis for MPN patients in general, see our separate webpage on this topic: recognising and preventing blood clots.
This risk is often caused by atherosclerosis which is a plaque build-up in blood vessels and blood vessel walls that can mainly affect the heart but can also affect the blood vessels of the brain and also the blood vessels of the legs.
Blood clots are the main cause of heart attacks and strokes in MPN patients as MPNs make the blood thicker, stickier, and more inflammatory than normal. Importantly, in MPNs there is also higher underlying chronic inflammation which leads to faster plaque build up and higher predisposing to plaque rupture.
Heart attack and MPN patients
A heart attack happens when a coronary artery (the vessels that feed the heart muscle) suddenly becomes blocked. The heart muscle downstream is starved of oxygen and starts to die. In MPNs, blockages can form even without plaques from cholesterol plaques. Mechanisms include:
- High red cell mass (especially in PV) causes sluggish blood flow
- Overactive platelets (especially in ET) causes clots form too easily
- Inflammation from the malignant clone (Jak2, CALR or MPL) so vessels become more “clot-friendly”, especially the Jak2 clone.
- Microclots can cause small vessels to be blocked.
An MPN patient can have a heart attack with normal or even low cholesterol.
MPN-related heart attacks may:
- Occur younger than expected
- Be silent or atypical (fatigue, breathlessness, jaw or back pain)
- Occur despite aspirin or “good numbers”
Most strokes in MPNs are ischemic strokes—a clot blocks blood flow to part of the brain. MPN patients are at higher risk of stroke because:
- Having the Jak2 mutation – (research shows that 11% of patients with an ischemic stroke have the Jak2 mutation although not all may have an MPN).
- Platelet activation can cause clots in cerebral arteries
- High haematocrit leads to poor microcirculation in the brain
- Abnormal clot breakdown means clots persist longer
- Small-vessel disease can cause repeated tiny infarcts over time
MPNs patients are also more prone to transient ischemic attacks (TIAs or mini-strokes), and also unusual stroke locations, including small cortical or deep brain vessels.
Especially in MPNs, strokes may show up as:
- Visual changes
- Word-finding difficulty
- Confusion or personality change
- Balance problems
- Migraines or “weird neurological episodes” that later turn out to be TIAs
Standard risk calculators underestimate MPN risk as they do not account for clonal hematopoiesis, platelet activation, or inflammatory thrombosis, which are central in MPNs.
Heart failure arises from either:
- systolic heart failure (caused by weakening of heart muscle and impaired pumping function), or
- diastolic heart failure (stiffness of heart muscle leading to impaired filling)
Symptoms are shortness of breath, swelling of legs, or abdomen, shortness of breath when flat, when tying shoes.
Importantly, MF patients may have other reasons that cause swelling of abdomen, leg swelling etc so it’s sometimes difficult to tease these out.
Over time, as the heart is damaged, it can cause kidney failure and/or liver failure, so it is important to identify and treat heart failure early to reduce risk of other complications.
Dr Orly Leiva’s research informs us that MPN patients are at increased risk for developing heart failure compared with the general population. And ‘among patients already at risk, such as those with acute coronary syndrome (heart attacks) or arrhythmias, those with MPNs have higher rates of heart failure hospitalisations’.
Myelofibrosis patients and heart failure
Myelofibrosis (MF) patients should be evaluated from a cardiologist in these situations.
How does heart failure tie in with MF?
A retrospective study showed patients with a more advanced form of MPN are at the highest risk of heart failure – eg a high WCC, large spleen. While there are not many studies yet available, Ruxolitinib seems to be associated with lower risk of heart failure.
Dr Leiva has just published in 2026, an article in Leukemia and Lymphoma titled ‘Ruxolitinib and heart failure outcomes among patients with myelofibrosis‘. It is freely available to access.
Interestingly, the research of Dr Leiva and team has showed that if PV and ET patients whose heart failure is serious enough to see the patient hospitalised – this should be a warning flag to haematologists to look out for disease progression in their MPN.
For more detail, an article published in 2025 and of which Dr Leiva is a lead author, sheds more light on this issue. Full access is available.
Beyond Thrombosis: Pulmonary Hypertension and Heart Failure in Patients With Myeloproliferative Neoplasms: JACC: CardioOncology State-of-the-Art Review
4. Pulmonary hypertension
Pulmonary hypertension means that blood pressure in the blood vessels of the lungs is too high. It is different from normal blood pressure as it is a specific problem with lung circulation.
In pulmonary hypertension, blood vessels in the lungs become narrow, stiff or blocked. This makes it more difficult for blood to move through, so pressure builds up. This means the right side of the heart has to work much harder to push blood into the lungs. And over time, that strain can cause: shortness of breath (especially on exertion), fatigue, dizziness or fainting, swollen ankles or legs, and chest discomfort.
As with congestive heart failure, pulmonary hypertension is not uncommon in MF patients
Dr Leiva’s article from late 2025, linked above, explains that pulmonary hypertension in particular has been linked to worse prognosis in patients with MPNs. And interestingly, it is also associated with increased risk for progression to either myelofibrosis or acute myeloid leukaemia.
Electricity problems include arrhythmias, atrial fibrillation (AF), heart block.
These should be evaluated by a cardiologist to determine best management.
The heart has its own built-in electrical system. If there are electrical problems and this signalling is disrupted, arrhythmias can occur. Arrhythmias are abnormal heart rhythms which can be intermittent or constant. They can be too fast (tachycardia), too slow (bradycardia) or irregular (fibrillation).
Electrical issues often overlap with pump or vessel disease in that they can reduce cardiac output; increase stroke risk (especially AF); cause sudden cardiac death; or often worsen other cardiovascular conditions.
Prevention and management of electrical issues might include: treating underlying heart disease; correcting electrolytes avoid triggers (stimulants, alcohol excess); prescribing medications to control rate or rhythm; anticoagulation when stroke risk is high; using devices (pacemaker, defibrillator) when needed.
A research article published in 2025 may be of interest to MPN patients with atrial fibrillation and the Jak2 mutation. Titled ‘Incidence, Outcomes and Risk Factors for Atrial Fibrillation in Patients With JAK2V617F-Positive Myeloproliferative Neoplasms‘ the full article is freely available from Cancer Medicine.
Managing cardiovascular risk factors in MPN patients
This section features two recommended approaches. The first from US cardiologist Dr Feldman. And the second from Australia’s haematologist, Dr Cecily Forsyth.
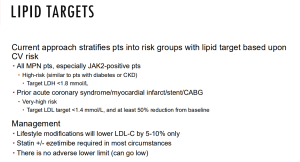
Prevention in MPN patients
- Under the management of a haematologist, control the blood counts
- Hematocrit control (especially in PV)
- Platelet control (especially in ET)
- Cytoreduction (interferon, hydroxyurea, etc.) or Jak inhibition when indicated
- Under the management of a haematologist -antithrombotic strategies
- Low dose aspirin for many patients (sometimes twice a day)
- Sometimes anticoagulation after a clot (This is highly individualized)
- Reduce inflammation, not just cholesterol
- Statins may help even with normal LDL, due to anti-inflammatory effects (see additional information on benefits of statins below)
- Recognize symptoms early
MPN patients should seek urgent care for:
- New neurological symptoms (even if transient)
- Chest discomfort that feels “off”
- Sudden breathlessness or unexplained fatigue
Dr Cecily Forsyth has prepared a range of information specific to MPN patients, and the additional measures that can be put in place by MPN patients’ care team to manage cardiovascular risk.
Below are some screenshots from her presentation but we also recommend watching or reading her whole presentation.
Statins?
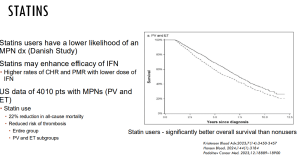
No randomised control trials of statins in MPNs exist, but some retrospective studies suggest that statins may be beneficial in reducing blood clots in MPN patients.
Dr Orly Leiva’s latest research on statins has concluded that ‘findings suggest that statins may provide meaningful cardiovascular protection in individuals with MPN, yet appear to be underutilized even among those with established clinical indications.’
And Danish MPN specialist haematologist Dr Hans Hasselbalch (also see below under ‘Inflammation’), has just published a review paper, explaining his view on statin use over the past two decades. Titled ‘Prime time for the use of statins in MPNs‘, it provides a basis for further discussion around health practitioners using statins in the care of MPN patients.
Inflammation and MPN patients
Part of managing cardiovascular health is also being aware of the fact that MPNs are very inflammatory.
This presentation by Dr Hans Hasselbalch at the same 2024 CR&T patient conference as Dr Feldman, outlines his thoughts on inflammation and MPNs.
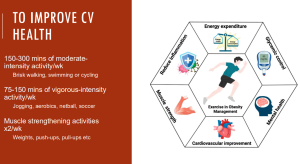
Exercise
And of course, of enormous benefit for cardiovascular health in MPN patients is exercise.
Important: Haematologists caution however to be sure to check with your GP and haematologist before launching on any new programme and start slowly and gently if you have not exercised before, or for some length of time.
THE ABCDE’s of cardiovascular health
This VIDEO PRESENTATION from US cardiologist Dr Stephanie Feldman was given specifically for MPN patients. It is available courtesy of the CR&T conference in October 2024 in the US.
In her presentation, Dr Feldman explains that ‘patients with cancer are at increased risk for cardiovascular disease. In order to protect your heart and prevent cardiovascular disease just follow the ABCDEs.’
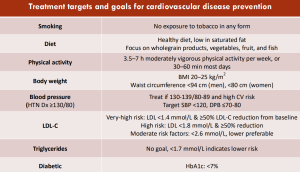
‘A= Awareness- it is important for you and your providers to be aware of the increased risk of cardiovascular disease and be on the lookout for symptoms such as chest pain, leg swelling, shortness of breath.
B= Blood pressure– Goal is less than 130/80. Know your numbers! If above goal follow a low salt diet, decrease alcohol, increase exercise, and talk to your doctor about medication.
C= Cholesterol- Goal is bad cholesterol (LDL) less than 100, lower if you have evidence of plaque on your heart arteries or have had a heart attack. This level should be checked once per year. Eat foods like avocado, olive oil, oatmeal to lower the LDL and talk to your doctor about medication like a statin if you are not at goal.
D= Diabetes– check bloodwork to screen for this at least once per year and make sure your average blood sugar over 3 months (hemoglobin A1c) is at your goal
E= Exercise! Goal is to work slowly up to 150 minutes of exercise per week (listening to your body) and 2 days of light weights.’ (NB. This must be done with the agreement of your doctor).
The above ABCDE’s are just an excerpt from her excellent presentation which we hope all MPN patients can find the time to watch.
Cardiovascular issues for MF patients
This webpage has outlined a number of cardiovascular issues that are especially important for MF patients, including heart failure and pulmonary hypertension. To summarise:
MF and heart failure
MF patients should be evaluated from a cardiologist in situations where there is a higher risk, such as those with a high white cell count and large spleen, acute coronary syndrome (heart attacks) or arrhythmias. A 2026 published article from Dr Leiva shows that ruxolitinib seems to be associated with lower risk of heart failure. ‘Ruxolitinib and heart failure outcomes among patients with myelofibrosis‘. It is freely available to access.
MF and pulmonary hypertension
Dr Leiva’s findings are that ‘clinical and preclinical data suggest a shared pathophysiology linking MPNs to the development and progression of cardiomyopathy, heart failure (HF), and ….. pulmonary hypertension (PH). Recent studies further support a bidirectional relationship, in which HF and PH are associated with hematologic progression and vice versa.’
For more detail, see Dr Leiva’s recent article. Full access is available.
Beyond Thrombosis: Pulmonary Hypertension and Heart Failure in Patients With Myeloproliferative Neoplasms: JACC: CardioOncology State-of-the-Art Review
And for a 2025 video presentation about MF and cardiovascular disease, see Dr Leiva’s presentation HERE.
Cardiovascular issues for PV patients
A detailed 2023 article from Italian haematologists outlined a number of cardiovascular issues for PV patients. Titled Diagnosis and management of cardiovascular risk factors in patients with polycythemia vera, it explains that modifying the cardiovascular risk profile in PV patients includes lifestyle modifications and pharmaceutical management of arterial hypertension and dyslipidemias (Dyslipidemia is elevation of plasma cholesterol, triglycerides, or both, or a low high-density lipoprotein cholesterol HDL level).
Australian Heart Foundation information about improving cardiovascular health
The Australian Heart Foundation has information at the links below about what is important for good cardiovascular health:
Are you at risk of heart disease?
The Australian Heart Foundation has further patient information available in several languages. The full selection can be accessed HERE.
